Understanding the Root Causes of Pelvic Health Imbalances
To effectively manage urge incontinence, it’s crucial to understand its underlying mechanisms. Unlike other forms of urinary leakage, urge incontinence primarily stems from an overactive bladder, often characterized by involuntary contractions of the detrusor muscle – the muscle responsible for emptying the bladder. These spasms can occur even when the bladder is not full, creating a sudden, compelling need to urinate that is difficult to postpone.
The communication between the bladder and the nervous system plays a significant role in this process. Sometimes, the nerves that signal bladder fullness and control its contractions become overactive or hypersensitive. This can lead to the bladder signaling a need to void prematurely or with excessive urgency. Factors contributing to this nervous system miscommunication can include neurological conditions, bladder inflammation, or even simply learned behaviors over time. For a deeper dive into the clinical understanding of these mechanisms, resources like the comprehensive review on Urge Incontinence from StatPearls offer valuable insights into the etiology and pathophysiology.
Additionally, hormonal changes, particularly the decline in estrogen during menopause, can impact bladder and urethral tissue health, potentially contributing to bladder hypersensitivity and weakening of the pelvic floor, exacerbating urge symptoms. Other contributing factors might include bladder hypersensitivity due to irritation from certain foods or drinks, or even structural issues within the bladder. Understanding these various “root causes” is the first step toward developing a personalized and effective treatment plan for managing this condition, as detailed in medical encyclopedias such as MedlinePlus’s guide to urge incontinence.
Differentiating Urge Incontinence from Stress Incontinenc
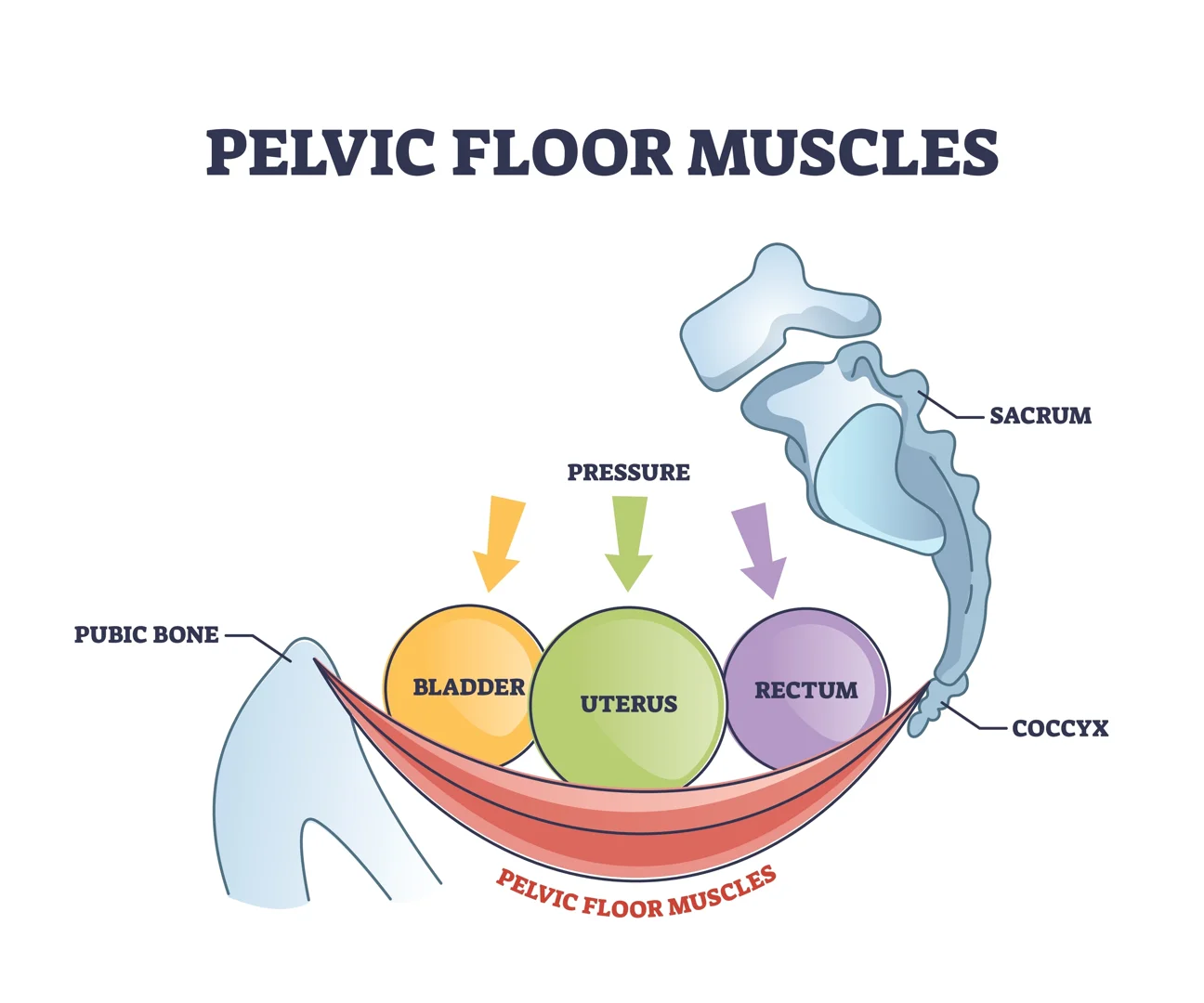
It’s important to distinguish urge incontinence from other types of urinary incontinence, particularly stress incontinence, as their causes and treatments differ significantly. Stress incontinence involves involuntary urine leakage caused by physical activity that puts pressure on the bladder, such as coughing, sneezing, laughing, or lifting heavy objects. This typically occurs due to a weakened pelvic floor or sphincter muscles.
In contrast, urge incontinence is characterized by that sudden, intense need to urinate, often resulting in leakage before reaching a toilet. This is not about physical pressure but rather an involuntary bladder contraction. Sometimes, individuals experience a combination of both, known as mixed incontinence. Understanding which type or types of incontinence you are experiencing is vital for accurate diagnosis and effective treatment.
For those seeking information on various types of bladder control issues and their treatments, including stress incontinence, local resources like the Idaho Urologic Institute can provide comprehensive guidance.
The Role of Diet, Hydration, and Bladder Irritants
What we consume daily significantly impacts bladder function. Concentrated urine, often a result of insufficient fluid intake, can irritate the bladder lining, triggering more frequent and urgent sensations. Paradoxically, excessive fluid intake can also overwhelm the bladder, leading to increased urgency and frequency. Finding the right balance is key. A simple guideline for optimal water intake is to divide your weight in pounds by two to determine the approximate number of ounces of water you should aim to drink daily. For instance, a 150-pound individual would aim for about 75 ounces.
Certain dietary components are known bladder irritants. Caffeine (found in coffee, tea, and some sodas), alcohol, acidic foods (like citrus fruits and tomatoes), spicy foods, and artificial sweeteners can all stimulate the bladder, increasing urgency and frequency. Reducing or eliminating these from your diet can often lead to a noticeable improvement in symptoms.
Furthermore, “just in case” voiding habits – urinating frequently even without a strong urge – can inadvertently train the bladder to hold smaller volumes, perpetuating the cycle of urgency. Your body isn’t failing you; it’s often responding to a combination of physiological factors and learned behaviors. Addressing these lifestyle elements is a powerful first step in regaining control.
Restoring the Pathways: First-Line and Behavioral Therapies
When addressing urge incontinence, we often begin with the least invasive yet highly effective strategies: behavioral and lifestyle interventions. These approaches empower individuals to take an active role in managing their symptoms and can significantly improve quality of life.

One cornerstone of behavioral therapy is bladder retraining. This involves gradually increasing the time between urination attempts, aiming to extend the bladder’s capacity and reduce the frequency of urges. Combined with urge suppression techniques – strategies to distract from or calm the urge when it arises – bladder retraining helps re-educate the bladder and brain connection. For detailed guidance on these and other first-line treatments for overactive bladder, authoritative medical sources like UpToDate provide clinical recommendations for females.
Lifestyle modifications also play a crucial role. Maintaining a healthy weight reduces pressure on the bladder and pelvic floor. Addressing chronic constipation, which can strain pelvic floor muscles and irritate the bladder, is also important. Simple changes like increasing fiber intake and ensuring adequate hydration can help. Quitting smoking, if applicable, is another beneficial step, as nicotine can irritate the bladder and chronic coughing can weaken the pelvic floor.
How Pelvic Health Physical Therapy Re-educates the Bladder
Pelvic health physical therapy is a specialized and incredibly effective non-pharmacological approach to urge incontinence. A trained pelvic floor physical therapist can provide personalized guidance on pelvic floor muscle training, commonly known as Kegel exercises. However, it’s not just about strengthening. A therapist can assess whether your pelvic floor muscles are too weak, too tight, or simply not coordinating properly.
Proper technique is paramount for Kegel exercises. Many individuals perform them incorrectly, which can be ineffective or even worsen symptoms. A physical therapist uses techniques like biofeedback, where sensors provide real-time feedback on muscle contractions, to ensure you are engaging the correct muscles. This helps in both strengthening weak muscles and teaching tight muscles to relax. The importance of these interventions is highlighted in clinical guidelines, such as those published in The Journal of Women’s & Pelvic Health Physical Therapy, which provide evidence-based recommendations for physical therapy management.
Beyond muscle strength and relaxation, pelvic health physical therapy addresses breathing control, posture, and body mechanics, all of which influence pelvic floor function. By re-educating the entire system, therapists help restore proper bladder function and reduce urgency symptoms.
Non-Invasive Electromagnetic Stimulation and HIFEM
In recent years, innovative non-invasive technologies have emerged to complement traditional pelvic floor rehabilitation. High-Intensity Focused Electromagnetic (HIFEM) technology is one such advancement. This therapy delivers electromagnetic waves that stimulate the pelvic floor muscles, inducing thousands of supramaximal contractions in a single session – contractions that are far more intense and effective than what can be achieved through voluntary Kegel exercises alone.
These powerful contractions help to rebuild and strengthen the pelvic floor muscles, improving their ability to support the bladder and control urges. The treatment is typically performed while fully clothed, and sessions are relatively short, often around 30 minutes. Patients often report an improved quality of life and a significant reduction in urge incontinence events. For those interested in learning more about how this technology works and its benefits, exploring options like HIFEM urge incontinence therapy can provide further details. This approach offers a convenient and effective option for many individuals seeking to enhance their pelvic floor strength and regain bladder control.
Advanced and Neuromodulation Options for Refractory Symptoms
When first-line behavioral therapies and lifestyle modifications do not provide sufficient relief, we may explore advanced medical treatments and neuromodulation options. These are typically considered for individuals with refractory overactive bladder – meaning their symptoms have not responded adequately to conservative measures.

One such option involves medications. Anticholinergics and beta-3 agonists are commonly prescribed to relax the bladder muscle, increase bladder capacity, and reduce the frequency and urgency of contractions. While effective for many, these medications can have side effects such as dry mouth, constipation, or blurred vision. A comprehensive overview of these and other treatments can be found in resources like the Mayo Clinic’s guide to urinary incontinence diagnosis and treatment.
For those who don’t respond to medications or experience intolerable side effects, minimally invasive procedures become an option. Botox injections into the bladder muscle can temporarily paralyze parts of the detrusor, reducing involuntary contractions and improving urge symptoms. The effects typically last for several months, requiring repeat injections. Sacral neuromodulation involves implanting a small device that sends electrical impulses to the sacral nerves, which control bladder function. This helps to normalize the communication between the brain and bladder, reducing overactivity.
Percutaneous Tibial Nerve Stimulation (PTNS)
Percutaneous Tibial Nerve Stimulation (PTNS) is another advanced neuromodulation therapy that is less invasive than sacral neuromodulation. This treatment involves placing a thin needle electrode near the tibial nerve, located just above the ankle. Mild electrical pulses are then delivered through the needle, traveling up the nerve pathway to the sacral nerves that control bladder function.
The theory behind PTNS is that these electrical impulses help to “jam” or modulate the abnormal nerve signals that contribute to bladder overactivity and urgency. It essentially helps to calm the overactive bladder nerves. Treatment typically involves a series of weekly 30-minute sessions for 12 weeks, with potential booster treatments thereafter. Many individuals experience significant improvement in their urge incontinence symptoms with this therapy. Exploring various advanced treatments for bladder control issues, including nerve stimulation, can be discussed with specialists at institutions like the Idaho Urologic Institute.
When to Seek Specialist Care for Pelvic Health Restoration
While many individuals find significant relief with first-line and behavioral therapies, there are times when seeking specialist care becomes essential. If you have persistent or worsening symptoms despite trying conservative measures, or if your symptoms are significantly impacting your quality of life, it’s time to consult a specialist such as a urologist, urogynecologist, or a pelvic health physical therapist.
A specialist can perform more in-depth diagnostic tests, such as urodynamic studies, which measure bladder pressure and urine flow, or a post-void residual volume test to check how much urine remains in your bladder after voiding. They can also rule out other underlying conditions that might be contributing to your symptoms. An interprofessional care team, including physicians and physical therapists, often collaborates to provide the most comprehensive and individualized treatment plan. Don’t hesitate to seek expert evaluation if you’re struggling to manage your symptoms; early intervention can prevent complications and significantly improve long-term outcomes.
Frequently Asked Questions About Bladder Control
We often encounter common questions from women seeking to understand and manage their urge incontinence. Here are some of the most frequent inquiries:
Does urge incontinence go away on its own?
Unfortunately, urge incontinence typically does not resolve on its own. While symptoms might fluctuate, the underlying patterns of bladder overactivity or nervous system miscommunication usually persist and can even worsen over time without intervention. Early intervention with behavioral therapies, lifestyle adjustments, and, if necessary, medical treatments, offers the best chance for significant improvement and long-term symptom management. Addressing the issue proactively helps prevent the condition from becoming chronic and more difficult to manage.
How do I know if my pelvic floor muscles are too tight or too weak?
This is a common and excellent question, as both overly tight (hypertonic) and weak pelvic floor muscles can contribute to urge incontinence. Weak muscles may not provide adequate support or control, while overly tight muscles can lead to bladder irritation, pain, and a constant sensation of urgency, mimicking a full bladder.
It’s challenging to self-diagnose muscle tone accurately. The best way to determine if your pelvic floor muscles are too tight or too weak is through a professional assessment by a pelvic health physical therapist. They can perform an internal examination to evaluate muscle strength, endurance, coordination, and the presence of any trigger points or excessive tension. Based on this assessment, they can then recommend appropriate exercises, which might include strengthening exercises if muscles are weak, or relaxation techniques and stretches if they are too tight.
What is the success rate of non-drug therapies for overactive bladder?
Non-drug therapies, particularly behavioral interventions and pelvic floor physical therapy, have a high success rate and are often recommended as first-line treatments due to their effectiveness and minimal side effects. Studies show that a significant number of patients experience substantial improvement in their urge incontinence symptoms with these approaches. For instance, bladder retraining combined with pelvic floor muscle training can lead to a 50% or greater reduction in urge incontinence episodes for many individuals.
Patient satisfaction rates are also high, as these therapies empower individuals to gain control over their bladder function without relying on medications. While success varies from person to person, the holistic integration of lifestyle changes, bladder retraining, and targeted pelvic floor exercises provides a robust foundation for long-term symptom reduction and improved quality of life.
Conclusion
The journey to managing urge incontinence is deeply personal, yet universally rooted in understanding and addressing the body’s intricate communication systems. We’ve explored how symptoms are not failures, but rather signals from an overactive bladder or a nervous system seeking balance. From foundational behavioral changes and the profound impact of pelvic health physical therapy to advanced neuromodulation techniques, a spectrum of effective therapies exists to restore confidence and control.
Living with constant urgency and leakage is not a life sentence. By taking an integrative approach, we can address the various facets of urge incontinence, from diet and hydration to muscle function and nerve signaling. We encourage you to view these insights not as a definitive end, but as an invitation to begin your own path toward pelvic health restoration. If you are experiencing symptoms, a calm, informed evaluation is your next best step. Exploring options to regain control and improve your daily life can be a truly empowering experience. To learn more about innovative treatments and take the first step towards a better bladder, consider exploring our resources on how our approach works or even booking an appointment for a personalized consultation.





